
During graduate school, I was obsessed with barefoot shoes—those thin-soled foot gloves with a separate pocket for each toe. I wore them everywhere: to research group meetings, to the grocery store, even to a formal dance. Regular shoes had always been uncomfortable. In toe shoes, my feet could finally stretch out. Then the pain started.
At first it was only a minor ache that I attributed to excessive standing. The ache worsened, until one day, I stood on the cold white tile of my home office and experienced sudden stabbing pain in both feet. The pain didn’t go away that evening, or the next day. I hobbled around on the outer edges of my feet trying not to put any pressure on the part that hurt. Finally, I booked an appointment with an orthopedic surgeon, wondering if had stress fractures.
The surgeon ordered x-rays, which are good for visualizing bones. I stood, with difficulty, while a technician imaged my feet from different angles. The surgeon glanced at the x-rays and informed me that because there were no fractures, my feet were fine. He sent me home.
I spent another few weeks miserably limping around until I decided to book an appointment with a podiatrist.
The podiatrist listened to my story about the barefoot shoes with a knowing expression, then did a physical exam of my feet to identify the exact location of the pain. He then did an ultrasound to look at the soft tissue, and there was the diagnosis: I had ruptured the joint capsules of my third and fourth metatarsophalangeal joints. I also found out that what I really needed wasn’t barefoot shoes, it was extra wide normal shoes. The podiatrist made me custom orthotics to take the weight off my damaged joint capsules. Wearing the orthotics inside my new extra wide running shoes felt like a miracle.
I wore the orthotics for years, outdoors and indoors with shoe covers, and the pain got better. But as soon as I tried to walk without the orthotics, the pain got worse again. I didn’t want to have to wear shoes inside for the rest of my life, so I decided to see a physical therapist. The physical therapist realized that my calf muscles were extremely tight, probably from the way I’d been walking while wearing the now-banished toe shoes. My tight calves were putting excessive pressure on my injured forefoot. I started an intensive stretching program for my calves. I can now walk barefoot and pain-free on a carpet or even—shockingly—on a tile floor.
This post is about diagnosis. The diagnostic process is not always linear, and different clinicians approach diagnosis through different lenses. Orthopedic surgeons focus on surgical problems of bones and joints, so when I didn’t have a surgical problem, that equated to “no problem.” The podiatrist correctly identified the diagnosis of ruptured joint capsules, but missed a contributing factor—my tight calf muscles, which can be thought of as a secondary diagnosis.
What goes on in a clinician’s mind when a patient walks in with a broad complaint like “foot pain”? Clinicians have several tools at their disposal: history-taking, physical examination, laboratory tests, imaging, procedural diagnostics, watchful waiting, and trials of treatment. During the remainder of this post, we will explore each of these tools in detail. Understanding the diagnostic process is relevant for health AI, because many health AI applications seek to augment or replace the human diagnostic process, with varying success.
Diagnostic Tool #1: History-Taking
“Listen to your patient. The patient is telling you the diagnosis.” This famous quote is often attributed to Sir William Osler, one of the most influential physicians in modern medicine and a founding professor of Johns Hopkins Hospital.
Here are some manufactured doctor-patient dialogues along with the diagnoses they suggest:
Patient: My pee is brown. It looks like Pepsi.
Doctor: When did it start?
Patient: After I ran a marathon. I hadn’t really trained for it but my roommate was doing it, so I thought, why not?
Suggests rhabdomyolysis, which can be triggered by high-intensity exercise. In rhabdomyolysis muscles release myoglobin into the bloodstream, which turns the urine brown.
Patient: I have this really strong urge to move my legs at night. It’s driving me crazy.
Doctor: Does anything make it better?
Patient: Getting up and walking around.
Suggests restless legs syndrome.
Patient: Sometimes I randomly lose consciousness and when I wake up, I have no idea what just happened.
Doctor: Does anything happen before these episodes?
Patient: Yeah. I smell burning rubber, or garbage.
Suggests temporal lobe epilepsy with olfactory aura. An “aura” is a warning sensation a person experiences before an attack of epilepsy or migraine.
You’ll notice that in these fake conversations the doctor asks a follow-up question intended to elicit additional specific information. This is “history-taking”: the process of asking questions to understand key details of the patient’s story.
History-taking ideally starts at the beginning of a visit with the doctor asking an open-ended question like, “What brings you in today?” Then the patient should have a couple minutes to talk, although studies have shown that doctors typically interrupt the patient after only 11 seconds. In this initial conversation, the patient reveals her chief complaints—her reasons for coming in.
Different medical specialties by definition attract different kinds of patients, so the distribution of chief complaints varies by specialty:
- Common chief complaints for an urgent care include cold symptoms, urinary issues, earache, eye infection, joint pain, muscle pain, stomach ache, rash, and genital symptoms.
- Common chief complaints for a dermatology clinic include acne, dry skin, cosmetic concerns, eczema, hair loss, nail changes, itching, psoriasis, seborrheic dermatitis, rash, and skin lesions.
When primary care doctors place referrals, and when receptionists book appointments, they help ensure that a patient’s chief complaints are appropriate for that specific clinic.
History-taking is not random. During history-taking, the doctor asks focused, strategic questions about each of the patient’s chief complaints. The skill of history-taking is explicitly taught in medical school and residency. Below are examples of common history-taking questions:
General history-taking questions that apply to all symptoms (e.g., replace the word “symptom” with headache, chest pain, shortness of breath, stomach ache, etc.)
- When did the symptom start?
- Does anything make your symptom better?
- What makes your symptom better?
- Does anything make your symptom worse?
- What makes your symptom worse?
- Is the symptom constant, or does it come and go?
- Do you have recurring episodes of your symptom?
- How long ago did you first experience your symptom?
- How long does an episode of your symptom last?
- How frequently do episodes of your symptom come on?
Pain history-taking questions
- Where is the pain located?
- How would you rate your pain right now on a scale of 1 to 10?
- When your pain is at its worst, how would you rate it on a scale of 1 to 10?
- Is the pain sharp or dull?
- How would you describe the pain?
- Does the pain travel anywhere else in your body (radiate)?
- Where does the pain go?
Example history-taking questions for a common chief complaint, headache
After asking the general questions and pain questions above:
- Do you have any vision changes, eye redness, eye watering, facial flushing, runny nose, ears ringing, numbness, weakness, nausea, vomiting, stiff neck, fever, or muscle pain?
- Do you get headaches at particular times of day?
- Do your headaches wake you from sleep up at night?
Another manufactured dialogue
Real history-taking often involve detours, ums, pauses, and conceptual side streets as the patient talks about his cat and where he’s going on vacation. Since a realistic dialogue would take up too many pages, instead let’s consider another manufactured conversation:
The chart tells the doctor that the patient is here for “headache.” The doctor walks in and sees a well-appearing, alert patient sitting upright in a chair laughing at something on his phone. The doctor immediately deprioritizes headache diagnoses that tend to cause debilitating pain, lethargy, or altered consciousness, like subarachnoid hemorrhage or bacterial meningitis.
This process, whereby initial visual observation of the patient affects the diagnoses under consideration, is technically part of the physical exam, a diagnostic tool we’ll talk about in the next section. I’m only mentioning it here because it affects the entire subsequent history-taking process.
Doctor: What brings you in today?
Patient: I keep getting these terrible headaches. I need them to go away.
Doctor: I’m sorry to hear that. When did these headaches start?
Patient: The one I have right now started yesterday. But I’ve been getting them for years.
The doctor begins considering diagnoses that cause chronic headaches.
Doctor: Does anything make your headaches better or worse?
Patient: I’ve tried Advil but it doesn’t really help. I know this is going to sound weird but I’m pretty sure grocery shopping makes them worse. I’ll be feeling fine and then I go to the grocery store and a few hours later, bam. Another headache. Sometimes I put off grocery shopping until there’s no food left in the house because I’m afraid I’ll get another headache.
Now the doctor is thinking about headaches that might be triggered by a grocery store environment. Migraines could be triggered by bright lights, strong smells (cleaning products, fish counter, perfumes), noise, or temperature changes in the frozen section. Cluster headaches could also be triggered by lights or smells.
Doctor: Could you tell me more about how the headache feels?
Patient: It’s throbbing all over.
Doctor: So it’s all over your head?
Patient: Yeah, it’s not really in one specific place. Maybe worse behind my eyes?
Doctor: And how bad would you say your pain is right now, on a scale of 1 to 10?
Patient: It’s like a six.
Doctor: When it’s at its worst, how bad does it get?
Patient: Maybe a nine?
Doctor: Any other symptoms? Nausea, sensitivity to light, vision changes? Teary eyes, runny nose?
Patient: I’m definitely nauseated. But I don’t have any of that other stuff.
Cluster headaches are often associated with one-sided pain, teary red eyes, runny nose, swollen or drooping eyelids, and restless agitation, so the above history makes cluster headaches somewhat less likely. Tension headaches are not stereotypically associated with nausea or throbbing pain. So, migraine is looking more likely after the above history.
Doctor: How long after the grocery shopping do your headaches come on?
Patient: It takes a couple hours. I went to the grocery store after work yesterday, got some takeout for dinner, and before I went to bed, my head was already hurting. And it was still hurting this morning.
Doctor: What did you have for dinner?
Patient: Salami lasagna, garlic bread, some weird banana tiramisu.
Doctor: Do you ever notice if certain foods trigger your headaches?
Patient: No. I mean I haven’t paid attention. I do usually get Italian when I go to the grocery store because the Italian place is right next to the grocery store.
Doctor: This sounds like it could be a migraine, possibly triggered by tyramine, which is high in cured meats like salami, aged cheeses like parmesan, and ripe bananas. I recommend you keep a food diary and record what you eat and when you get headaches, so we can check if there’s a connection. In the meantime, I’ll prescribe you some anti-migraine medication…
The above example is contrived, but hopefully conveys the dynamic in which the doctor asks targeted questions and progressively changes the mental probability of different diagnoses as the patient responds.
History taking across specialties
History-taking is more important in some specialties than others. Psychiatry and medical genetics are especially history-focused, and often write long notes as a consequence. Pathology, in contrast, is based on interpreting images of cells under a microscope, and while the pathologist has access to the patient’s clinical notes, she does not take a history from the patient directly.
Structured questionnaires as part of history-taking
Validated structured questionnaires can be part of history-taking. For example, the PHQ-9 is a nine-question self-report measure for screening and measuring depression severity. It asks about frequency of symptoms like low mood, loss of interest, and sleep problems, occurring not at all (0 points), several days (1 point), more than half the days (2 points), and nearly every day (3 points). The total number of points ranges from 0 to 27 and indicates the severity of depression symptoms. Validated questionnaires like the PHQ-9 are often administered before appointments so that the results can be discussed during the appointment if needed.
History-taking as an algorithm
From one perspective, history-taking is purely algorithmic. The questioning process is based on an underlying tree data structure. For a chief complaint like headache, the root of the tree is a general question asking about the presence of the chief complaint, e.g., “Do you have a headache?” An affirmative response triggers the next level of questioning, which are questions like the ones shown above: “When did the headache start?” “Does anything make the headache better?” and so on. As the doctor traverses the question tree, she gets more and more information needed to determine the diagnosis. History-taking can be automated, and indeed, at my startup Cydoc, we built a software platform for automated history-taking.
From another perspective, history-taking is an art. The process of history-taking through a real-life conversation involves weaving questions together into a coherent conversation, while gently redirecting the patient after they go off on a tangent, while expressing empathy. Marketing automated history-taking to doctors requires extremely careful phrasing, to avoid offensively undermining a clinician’s sense of her own artistry.
Foot injury example
In my foot injury saga, the relevant history was concise: I had worn barefoot shoes and experienced progressive pain that culminated in a specific incident where the pain got much worse. This history is consistent with joint capsule inflammation followed by rupture, but the story isn’t sufficient for diagnosis on its own. Physical exam and imaging also proved necessary. In the next section, we’ll explore the physical exam.
Diagnostic Tool #2: Physical Examination
Vital signs
The four standard vital signs and their normal ranges are:
- Heart rate (pulse): 60 to 100 beats per minute
- Respiratory rate: 12 to 18 breaths per minute
- Blood pressure: between 90/60 mmHg and 120/80 mmHg
- Temperature: 97.8°F (36.5°C) to 99.1°F (37.3°C); average 98.6°F (37°C)
Additional measurements sometimes reported with vital signs include:
- Oxygen saturation (SpO2): 95 to 100%
- Pain level: 0 (no pain) to 10 (worst pain)
- Height, weight, and body mass index
Abnormal vital signs are critical clues for diagnosis.
- Heart rate
- Too fast (>100 bpm, aka tachycardia): can be seen with exercise, pregnancy, pain, fever, infection, shock, dehydration, panic attacks, caffeine use, high thyroid hormone, anemia, low blood pressure, certain electrolyte imbalances, and heart electrical issues.
- Too slow (<60 bpm, aka bradycardia): can be normal in athletes, or can signal medication side effects, low thyroid hormone, increased pressure inside the head, inflammation of the heart muscle, and heart electrical issues.
- Heart rate abnormalities accompanied by symptoms like chest pain, dizziness, or shortness of breath require immediate medical attention.
- Respiratory rate
- Too fast (>20 bpm, aka tachypnea): can be caused by pneumonia, asthma, COPD exacerbation, blood clots in the lungs, or compensation for acidic blood.
- Too slow (<12 bpm, aka bradypnea): can be caused by opioid overdose, sedatives, certain neurological conditions, or severe fatigue from respiratory muscle exhaustion.
- Pattern and effort of breathing matter too: e.g., shallow vs. deep breathing.
- Blood pressure
- Too high (>130/80, aka hypertension): if chronic, can be its own diagnosis. Severely elevated blood pressure is an emergency requiring immediate treatment.
- Too low (systolic <90, aka hypotension): can be caused by dehydration, bleeding, severe infection, heart failure, or medication effects.
- The difference between the systolic (first number) and diastolic (second number) pressures is called the pulse pressure. Wide or narrow pulse pressure has specific causes. A drop in blood pressure of >20 mmHg systolic when going from sitting to standing is referred to as orthostatic hypotension and can be caused by low body fluid volume or by nervous system dysfunction.
- Temperature
- Too high (>38°C/100.4°F, aka fever or hyperthermia): can be caused by infection, inflammatory conditions, cancer, drug reactions, or heat stroke.
- Too low (<35°C/95°F, aka hypothermia): can be caused by exposure to cold, infection, low thyroid hormone, or low blood sugar.
- The pattern of fever is important. Sustained fever suggests conditions like pneumonia, while intermittent or cyclical fevers could indicate conditions like malaria, tuberculosis, or lupus.
Vital sign abnormalities are always interpreted in the clinical context, including the patient’s history, symptoms, and other physical exam findings.
For blood pressure especially, it’s critical to compare the patient’s current blood pressure against their baseline blood pressure. A blood pressure of 100/65 is great if the patient’s baseline is 95/60—the minor difference of a few mmHg is within normal blood pressure variation, and this represents an unchanged, healthy blood pressure. But that same blood pressure of 100/65 would be alarming if the patient has chronic uncontrolled high blood pressure with a baseline of 200/110. In that case, the blood pressure of 100/65 is alarmingly low and should trigger thinking about causes and management of low blood pressure.
Example physical exam
In a general physical exam, the doctor examines the patient’s overall appearance, heart, lungs, head, eyes, ears, nose, throat, abdomen, limbs, skin, pulses, and reflexes. Every doctor has their own order of examining body parts, and their own definition of what constitutes a routine physical exam. I’ll describe one way of doing a physical exam, along with examples of some of the information a doctor could glean from it.
First, the doctor observes the patient’s general appearance. The patient’s general appearance conveys a lot of information. Consider the differences between these patients:
- An athletic young man in hockey gear with his forearm bent at a terrible angle;
- An ill-appearing, lethargic old woman with yellowed skin suggesting liver disease;
- An agitated, unwashed man pacing the room, muttering to himself;
- A little girl curled up on her side on the exam table;
- A pregnant middle-aged woman sitting quietly with her hands in her lap.
The doctor obtains a massive amount of information simply by looking at the patient for a few seconds. (This automatic, at-a-glance analysis is something that large language model chatbots are missing, making it harder for them to interact with patients safely.)
Let’s consider Dr. Alice examining patient Bob for a routine annual physical.
The doctor takes out a stethoscope and listens to the front of the chest. She is listening to the heart.
- A normal heartbeat has a regular lub-dub sound.
- An abnormal heartbeat might be too fast, too slow, the wrong rhythm, or include extra sounds.
- A too-fast heartbeat is called tachycardia, and a too-slow heartbeat is called bradycardia. Example causes are listed in the section on Vital Signs.
- An arrhythmia is an abnormal heart rhythm. Arrhythmias can originate from the heart’s upper chambers, the atria, or from the heart’s lower chambers, the ventricles. One type of atrial arrhythmia is atrial fibrillation, which creates a heartbeat that sounds irregularly irregular.
- The doctor can also hear heart murmurs, which are caused by rough flow of blood. The doctor can tell what anatomical part of the heart is causing the murmur based on the murmur’s quality, volume, location, timing within the heartbeat, and whether it gets better or worse with certain maneuvers. For example, if a patient has a heart murmur that increases in intensity when the patient bears down (Valsalva maneuver), this suggests hypertrophic cardiomyopathy, a condition where the heart muscle is abnormally thickened.
The doctor then listens to the patient’s back with her stethoscope and asks the patient to take deep breaths. She is listening to the lungs.
- Normal breath sounds are fresh and clear.
- Abnormal breath sounds include wheezes, rales, and rhonchi.
- Wheezes are high-pitched whistle-like sounds that can be heard in asthma, chronic obstructive pulmonary disease, or accidental lodging of an object in the airways.
- Rales, also called crackles, are light popping or crackling sounds, like Rice Krispies cereal. They can be heard in heart failure, pneumonia, interstitial lung disease, collapsed lung tissue, and acute respiratory distress syndrome.
- Rhonchi are low-pitched rumbling, snoring-like, or gurgling sounds that can be seen in bronchitis, pneumonia with thick secretions, or any condition that results in excessive mucus production.
Next the doctor looks at the eyes:
- She shines a penlight in the patient’s eyes to check that the pupils get smaller in response to light.
- The doctor asks the patient to follow her fingers with his eyes, going up, down, right, left, and diagonally. This checks if all of the muscles that move the eye are working.
- The doctor may move her fingers close to the patient’s face, to check if the patient’s pupils get smaller when he looks at something close by.
- The doctor checks visual acuity with an alphabet chart that has letters of different sizes (Snellen chart).
- She checks peripheral vision by asking the patient to look straight ahead and say the number of fingers she’s holding up in the corners of his vision.
Collectively, these parts of the physical exam check the function of cranial nerves II, III, IV, and VI. The cranial nerves are special nerves that originate from the brain and pass through tiny openings in the skull to the head, neck, chest, and abdomen. Problems with cranial nerves can be due to specific brain issues or issues with the nerves themselves. Depending on the particular constellation of abnormalities, it can be possible to pinpoint a particular brain region that has been damaged by a disease process like a stroke.
Next, the doctor asks the patient to stick out his tongue, say “aah,” and swallow. The patient’s tongue should stick out midline, and not deviate to one side or the other, the patient’s palate should lift symmetrically, and he should be able to swallow. This checks cranial nerves XII, IX, and X.
The doctor feels the patient’s neck.
- The doctor can feel if the patient’s thyroid is enlarged, as may be seen in iodine deficiency or certain thyroid diseases like Grave’s disease.
- The doctor can also feel if lymph nodes are enlarged, which is often seen with infections, like colds or strep throat.
The doctor checks the patient’s hearing by asking the patient to close his eyes and listen for a soft sound like whispering or fingers rubbing together.
- Hearing loss can be conductive, caused by problems in the outer or middle ear that block sound, or it can be sensorineural, caused by problems with the inner ear or auditory nerve. There are additional physical exam maneuvers using tuning forks that can be used to distinguish conductive from sensorineural hearing loss.
With an oto-ophthalmoscope, the doctor looks inside the patient’s ear.
- Eardrum inflammation can be seen in ear infections.
- Excessive wax is a common cause of diminished hearing.
The doctor also uses the oto-opthalmoscope to look inside the eye, at the retina, optic disc, and blood vessels, which can be abnormal in glaucoma, high blood pressure, diabetes, or high pressure inside the head.
The doctor asks the patient to lie flat.
- The doctor listens to the patient’s belly for bowel sounds.
- Excessive bowel sounds (called borborygmi, which is a wonderful word), can be heard in normal digestion, or with diarrhea, food intolerances, or inflammatory bowel disease.
- Absent bowel sounds in certain clinical context can suggest bowel obstruction, severe inflammation, or paralytic ileus, a condition where the intestinal muscles do not move.
- The doctor feels the patient’s belly, searching for abnormalities like masses (from hernias, cancer, or other causes), tenderness, guarding (tensing of the muscles to guard against pressure-induced pain), an enlarged liver (e.g., seen with liver infections like viral hepatitis, or liver diseases like cirrhosis), or an enlarged spleen (e.g. seen with infections like mononucleosis or malaria).
The doctor inspects the patient’s skin looking for any rashes or moles. In dehydration, the skin may remain peaked when lightly pinched, referred to as tenting.
The doctor checks the ankles for swelling (edema) which can be seen in chronic venous insufficiency, injuries, pregnancy, blood clots, heart disease, or kidney disease.
The doctor uses her fingertips to feel the strength and rate of peripheral pulses, like the radial pulse at the wrist.
The doctor uses a reflex hammer to tap the knee, checking if the patellar tendon reflex is normal, reduced, or excessive.
- Reduced reflexes can be caused by damage to lower motor neurons.
- Excessive reflexes can result from electrolyte imbalances or damage to upper monitor neurons in the brain or spinal cord.
But wait, there’s more…
Multiple textbooks have been written entirely about the physical exam. Like medicine as a whole, the physical exam is both a science and an art, and there are hundreds of different physical exam maneuvers that can be used for diagnosis. Here are a couple examples:
- If the doctor asks the patient to flex his neck, and the patient experiences an electric shock sensation that radiates down his spine, this is suggestive of multiple sclerosis, and is referred to as Lhermitte’s sign.
- If the doctor presses into the right upper part of the belly while the patient inhales, and the patient abruptly stops inhaling (due to pain), this suggests gallbladder inflammation, and is referred to as Murphy’s sign.
Specialty-specific exams have significantly more detail for the specialty-relevant body system. For example, an ophthalmologist will carry out a much more detailed eye exam, a dermatologist will carry out a much more detailed skin exam, and a cardiologist will carry out a much more detailed heart exam.
Some conditions can be diagnosed based on physical exam alone, including certain injuries, infections, skin conditions, and heart conditions.
The senses
The doctor leverages her senses of sight, hearing, and touch to carry out a physical exam.
Smell is occasionally relevant, e.g. an acetone smell suggesting diabetic ketoacidosis, a musty or garlic odor suggesting liver disease, or a foul odor from a wound suggesting infection.
In the old days, doctors would unfortunately taste a patient’s urine. If it tasted sweet, this suggested diabetes. I suspect that if drinking patient urine were a requirement to enter medical school, there would be far fewer applicants.
Tools of the trade
In the example physical exam above, the doctor used a stethoscope, penlight, oto-ophthalmoscope, reflex hammer, and Snellen chart.
There are numerous other pieces of equipment that doctors can use in a physical exam. Ophthalmologists may use a slit lamp and tonometer. Otolaryngologists may use a nasal speculum. Neurologists may use a monofilament. Dermatologists may use a dermatoscope and Wood’s lamp. Obstetricians and gynecologists may use a speculum or colposcope.
Patient respect
It is important for a doctor to wash her hands before beginning the exam, verbally guide the patient through what is happening, and use cloth or paper drapes to ensure the patient is not left unnecessarily exposed. For exams of sensitive areas the doctor should always have a chaperone in the room, often a nurse. It can be helpful for the patient if the doctor states her conclusions about different components of the exam, noting aloud what looks normal or abnormal.
Foot injury example
The orthopedic surgeon did not do much of a physical exam on my foot, and instead opted for an x-ray. The podiatrist did do a physical exam, inspecting the exteriors of my feet before pressing on them systematically to identify the exact location of the pain. This physical exam determined the first place that the podiatrist looked with the ultrasound. The physical therapist also did an exam, focused on my joints and muscles, and identified the calf tightness that was contributing to the foot injury’s persistence.
Diagnostic Tool #3: Laboratory Testing
History and physical exam can sometimes be sufficient for diagnosis, but other times, more information is needed. One common way to obtain more information is through a lab test.
Lab tests can be based on a wide range of body substances including blood, urine, tissue, cerebrospinal fluid, amniotic fluid, phlegm, saliva, stool, sweat, breast milk, and bone marrow. Lab tests are used for diagnosis of infections, electrolyte imbalances, hormone disorders, autoimmune disease, cancer, heart problems, liver problems, kidney problems, blood disorders, brain disorders, gut disorders, metabolic disorders, poisoning, drug overdoses, and more.
The WHO maintains a list of approximately 100 essential laboratory tests, but the scope of available tests in the United States is much vaster than this. There are more than 100,000 different kinds of laboratory tests, based on a huge range of underlying technologies including spectroscopy, chromatography, enzyme-linked immunosorbent assay (ELISA), DNA sequencing, microscopy, and more.
Common lab tests
Common lab tests include a basic metabolic panel (BMP), comprehensive metabolic panel (CMP), complete blood count (CBC) with differential, lipid profile, thyroid tests, and urinalysis. Some lab tests can be run at home, like pregnancy tests and covid tests.
Specialty-specific lab tests
There are all kinds of specialty-specific laboratory tests. For example, the specialty of medical genetics often uses whole-exome sequencing (WES, pronounced “wess”), which refers to DNA sequencing of the parts of the DNA that code for proteins. The fact that WES can be routinely ordered is a testament to the speed of scientific progress. The Human Genome Project, concluding in 2003, cost $2.7 billion, but a whole exome sequence or whole genome sequence costs only a few hundred dollars today.
Lab tests in clinical context
Clinical context determines which lab tests a clinician orders. Lab tests are always ordered to answer a specific clinical question. Let’s consider a couple examples:
| Clinical context | Clinical question | Lab test that could help answer the question |
| Abnormal heart rhythm on exam | Does this patient have an electrolyte abnormality as the underlying cause of her arrythmia? | BMP (Na, K, Cl), Mg, Ca, phosphate |
| Known end-stage renal disease (ESRD) | Is this patient’s kidney function stable or worsening? | BMP (creatinine, BUN) |
| Decreased urine output, nausea, and leg swelling | Does this patient have acute kidney injury? | BMP (creatinine, BUN) |
| Increased thirst and family history of diabetes | Does this patient have diabetes? | Blood glucose |
| Weight gain, dry skin, dry hair, puffy face, slow heart rate on exam | Does this patient have low thyroid hormone (hypothyroidism)? | Thyroid hormone tests |
| Missed menstrual period | Is the patient pregnant? | Pregnancy test |
After the lab test results are available, the results are interpreted in the clinical context. For certain lab tests, the patient’s baseline values are a key aspect of result interpretation, just like blood pressure discussed in the Physical Examination section. A creatinine of 1.4 could represent acute kidney injury in an otherwise healthy patient with a baseline creatinine of 0.9, while a creatinine of 1.4 could actually represent a “good” creatinine in a patient with chronic kidney disease and a baseline creatinine of 1.6.
Now, we’ll consider the BMP lab test in more detail.
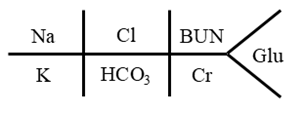
Basic Metabolic Panel (BMP)
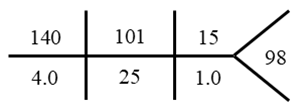
A BMP is typically handwritten with a fishbone structure:
Example with values:
The four electrolytes measured are:
- Sodium (Na)
- Chloride (Cl)
- Potassium (K)
- Bicarbonate (HCO3)
There are two markers of kidney function:
- Creatinine (Cr)
- Blood urea nitrogen (BUN, read as B-U-N, not “bun.”)
Glu indicates blood glucose, which is blood sugar.
Interpreting the BMP for Electrolyte Balance
The BMP provides insight into a patient’s electrolyte balance. Here is an example with sodium:
Sodium (normal 135 to 145 mEq/L)
- Low sodium (<135):
- Excess water: excessive water intake, SIADH
- Sodium loss: vomiting, diarrhea, nasogastric tube suction, medicines that cause sodium loss, adrenal gland insufficiency
- Low effective circulating volume: heart failure, liver cirrhosis, nephrotic syndrome
- High sodium (>145):
- Water deficit/water loss exceeds sodium loss: inadequate water intake, watery diarrhea, diabetes insipidus
- Sodium gain: salt poisoning
Differential diagnoses like those shown above are also available for low/high chloride and for low/high potassium.
Interpreting the BMP for Kidney Function
The BMP also provides insight into the patient’s kidney function, via the BUN and creatinine.
Most often, the abnormality seen with BUN and creatinine is that they are too high, often seen in kidney disease, although elevated BUN and creatinine can also be seen with dehydration, high-protein diets, high muscle mass, or increased muscle breakdown.
With elevated BUN and creatinine, the BUN-to-creatinine ratio tells a story:
- A ratio of >20:1 suggests a prerenal (“before the kidney”) issue like dehydration, heart failure, or a gastrointestinal bleed.
- A ratio of 10 to 20:1 can be normal or a postrenal (“after the kidney”) issue.
- A ratio of <10:1 suggests intrarenal (“within the kidney”) disease, liver disease, or malnutrition.
It’s also possible for BUN or creatinine to be too low, although this is rare. Low BUN and creatinine can be caused by malnutrition, a low-protein diet, liver disease, pregnancy (due to increased kidney function), and certain muscle disorders.
Interpreting the BMP for Blood Sugar Regulation
The glucose value of the BMP provides insight into the patient’s blood sugar regulation. Glucose should be interpreted in context:
- Does the patient have known diabetes?
- What’s the glucose trend over time/comparison to baseline?
- Was the patient fasting or not fasting at the time of the lab?
A glucose of 130 could be high for one person, if it’s a fasting glucose and their previous measurement was 90. But that same glucose of 130 could be low for another person, if they have diabetes and their glucose is normally at 170. Low glucose can be seen with excess insulin, severe illness, and starvation. High glucose can be seen with diabetes, stress (from acute illness, trauma, stroke, heart attack, and surgery), certain medications, and hormonal disorders.
Interpreting the BMP for Acid-Base Status
A BMP can be leveraged alongside an Arterial Blood Gas (ABG) for a sophisticated analysis of the patient’s acid-base status. This is a complex analysis involving multiple equations, and is outside the scope of this post, but interested readers can refer to Acid-Base Analysis: A Comprehensive Step-by-Step Approach for ABG and BMP Interpretation.
What a lab test doesn’t tell you
Doctors do not only think about what a lab test does tell them—they think about what it doesn’t tell them. Consider a lab test that on the surface seems very simple: a pregnancy test. The presence of a colored stripe on a pregnancy test diagnosis a pregnancy. But it doesn’t tell you how far along the pregnancy is, or if the pregnancy is located in the uterus. It doesn’t distinguish between a healthy singleton pregnancy, an embryo with a fatal chromosomal abnormality, a molar pregnancy, or a multiple pregnancy. Lab tests are powerful, but also only one tool in the diagnostic arsenal. In the pregnancy example, if we want to know about pregnancy dates, location, multiples, or molarity, we need ultrasound: a type of medical imaging.
Diagnostic Tool #4: Medical Imaging
Medical images provide stunning views of the human body, and they are an especially promising area for health AI due to the incredible power of computer vision. There are hundreds of different variations to medical images: not only is the modality specified (x-ray, CT, MRI, ultrasound), but also the use of injected or swallowed contrast, the timing of contrast, the body part of interest, and the angles or “views” of interest, all of which affect the image’s diagnostic utility. This section will focus on radiologic medical images, specifically x-rays, CT scans, MRIs, and ultrasounds. This is distinct from other kinds of medical images, like images taken via an endoscope, photographs of a patient’s skin, or histopathologic images obtained with a microscope.
X-rays are 2D black-and-white photographs obtained by shining x-rays through a body part. X-rays are fast, cheap, and safe. Limb x-rays are great for detecting fractures and joint problems. Chest x-rays can depict heart enlargement, pneumonia, emphysema, and rib fractures. However, x-rays do not effectively depict soft tissues or overlapping structures. Also, because x-rays are static two-dimensional images they cannot be used to evaluate flow or motion.
CT scans are 3D black-and-white images obtained by shining x-rays through a body part with a rotating machine that computationally reconstructs a 3D representation of the target body parts. CT scans display beautiful details of internal structures via fine-grained cross-sectional views. CT scans are fast, and thus ideal for emergency situations and trauma. They are good for detecting bleeding, tumors, and complex fractures, and can be used to image the entire body quickly. However, CT scans provide higher ionizing radiation exposure than 2D x-rays, and some CTs involve swallowed or injected liquid contrast material that can cause allergies. CT scanners are expensive to purchase and maintain.
MRIs are 3D black-and-white images obtained using strong magnetic fields. For readers with a chemistry background, MRI for medical purposes is based on the exact same technology as nuclear magnetic resonance (NMR). In fact, MRI for imaging patients was almost named “NMRI” or “nuclear magnetic resonance imaging” but then some wise person with marketing savvy decided to drop the word “nuclear” because that would scare patients. Ironically, although “nuclear” magnetic resonance imaging sounds like it would be radioactive, MRI doesn’t involve any ionizing radiation at all.
MRIs are excellent for soft tissue analysis, and are especially good at depicting the brain, spine, and joints, including visualization of organ function and blood flow. However, they are extremely expensive and slow, requiring 30 to 90 minutes per scan, they cannot be used if the patient contains metal implants or certain types of pacemakers. They can be unpleasant for claustrophobic patients due to their small interior dimensions.
Ultrasounds are black-and-white videos, sometimes with bright colors superimposed to demonstrate directionality of blood flow. Ultrasounds are obtained by sending ultrasonic sound waves into a body part and listening for the echoes, like a bat’s echolocation. Ultrasounds allow for real-time imaging, showing movement and flow. They are portable, cheap, and involve no ionizing radiation. Ultrasounds are ideal for pregnancy monitoring, heart function evaluation (a heart ultrasound is called an echocardiogram), and for guided procedures like kidney biopsies. However, ultrasounds are extremely operator-dependent, meaning the ultrasound technician’s skill level vastly affects how clinically useful the images are. Ultrasonic waves also cannot penetrate bones or gas-filled organs like the lungs, and ultrasounds have limited depth and quality in more obese patients.
There isn’t a single kind of medical image that is superior to all others. Each kind of medical imaging has its own strengths and weaknesses, which is why all types of medical imaging are used in different contexts.
Radiation
Ionizing radiation is the scary kind of radiation that comes out of nuclear bombs, and also x-ray machines and CT scanners, but in much lower doses.
A single chest x-ray is extremely safe, delivering only 0.1 mSv of radiation, equivalent to 10 days of natural background radiation, which is the radiation you are exposed to simply by being alive. Background radiation comes from cosmic rays, radioactive materials in the Earth’s crust, and radon gas. Eating a single average-sized banana exposes a person to about 0.1 μSv of radiation, because of the potassium.
CT scans are also safe, but involve slightly more radiation exposure. A low dose chest CT scan, e.g. for lung cancer screening, delivers about 1.5 mSv of radiation, equivalent to about 6 months of background radiation. Getting one CT scan is safe, but you probably should not go out there and get yourself 100 CT scans in a row. I did once meet a patient who enjoyed getting CT scans and repeatedly presented to the emergency department describing symptoms that sounded like ruptured aortic aneurysm, buying himself close to 50 CT scans, which is absolutely not a good idea. Don’t be that guy.
Magnets
The magnets used in MRI machines are extremely strong, with the ability to turn otherwise harmless metal into lethal projectiles. Absolutely no magnet-responsive metal is permitted in an MRI room, but humans being human, they sometimes make mistakes, so you can find crazy videos online of office chairs and oxygen tanks hurtling through the air into the mouth of an MRI. It’s especially dangerous if the stray metal is inside the patient’s body to begin with, e.g. because they’ve got leftover bullet fragments inside, piercings, or a medical implant or pacemaker. That is why before a patient gets an MRI, they are asked multiple times by multiple people if they have any metal in their body.
Foot injury example
When I injured my foot, the orthopedic surgeon used an x-ray to look for fractures, while the podiatrist used an ultrasound to look at my joint capsules. This is appropriately leveraging the strengths of these different kinds of medical images.
Diagnostic Tool #5: Procedural Diagnostics
Procedural diagnostic tests involve invasive or interventional procedures. Some procedural diagnostic tests are both diagnostic and therapeutic, meaning they can help clinicians pinpoint a diagnosis but also treat the patient at the same time.
Procedural diagnostics that are both diagnostic and therapeutic
An endoscopic procedure (“-oscopy”) uses a flexible camera to look inside hollow body parts. Endoscopic procedures can be used therapeutically to remove concerning tissue or objects, and/or to repair damage.
- A bronchoscopy is used to inspect the airways for infectious, tumors, and inhaled objects.
- An upper endoscopy is used to inspect the esophagus, stomach, and first part of the small intestine for ulcers, bleeding, or tumors.
- A sigmoidoscopy examines the lower colon.
- A colonoscopy is more extensive than a sigmoidoscopy. It inspects the entire colon for polyps and tumors.
- A cystoscopy is used to inspect the urethra and bladder for stones and tumors.
- A hysteroscopy is used to inspect the inside of the uterus to investigate structural abnormalities, polyps, scars, or cancer.
- A laparoscopy is used to inspect the inside of the abdomen and pelvis to investigate problems with the organs of digestion and reproduction.
- An arthroscopy is used to inspect the inside of a joint to diagnose cartilage tears or joint damage.
Cardiac procedures focus on the heart—a dynamic hollow body part filled with blood and constantly moving.
- Cardiac catheterization involves threading a catheter through blood vessels into the heart to evaluate heart function or to diagnose and treat heart vessel blockages. The heart has its own blood vessels, and when these become blocked it causes a heart attack.
A biopsy involves removing a solid tissue sample from a solid body part.
- A needle biopsy extracts a needle-thin piece of tissue, for example from a suspicious mass in the breast, liver, or kidney.
- A fine needle aspiration sucks up cells, rather than tissue chunks, from thyroid nodules, lymph nodes, or soft masses, often to help with diagnosis of cancer.
- A bone marrow biopsy is used for diagnosis of blood disorders, cancers, or infections.
- A skin biopsy helps diagnose skin disease and skin cancer. Excisional skin biopsies can be curative, if the whole diseased area is removed during the biopsy.
An aspiration procedure (“-centesis”) involves removing a fluid sample for analysis. Aspiration procedures can be therapeutic by relieving pressure caused by excess fluid.
- A lumbar puncture removes cerebrospinal fluid from the spine for diagnosis of meningitis, bleeding, or other conditions.
- A thoracentesis removes fluid from around the lungs to diagnose infections, cancer, or heart failure.
- A paracentesis removes fluid from the belly to investigate liver disease, cancer, or infections.
- An arthrocentesis removes joint fluid to investigate infection, inflammation, crystal-induced arthritis, and bleeding.
- A pericardiocentesis removes fluid from the sac around the heart to help diagnose infection, cancer, and inflammation.
- An amniocentesis removes fluid from the amniotic sac during pregnancy to diagnose fetal conditions.
As noted in the header, all of the aforementioned procedures could have a therapeutic aspect. There are also some procedural diagnostics that are purely diagnostic, which we will discuss next.
Procedural diagnostics that are diagnostic-only
An electrophysiologic study measures electrical activity of a body system.
- An EKG/ECG (electrocardiogram) traces the electrical activity of the heart to help diagnose abnormal heart rhythms and heart attacks.
- An EEG (electroencephalogram) traces the electrical activity of the brain to help diagnose seizures.
- An EMG (electromyogram) traces the electrical activity of a muscle to help diagnose disorders of nerves and muscles.
Functional studies quantify the function of a specific body part.
- Pulmonary function tests measure lung capacity and airflow.
- Esophageal manometry measures esophageal muscle contractions and pressure.
- Anorectal manometry evaluates anal sphincter function.
- Urodynamic studies evaluate bladder function and urinary incontinence.
Challenge tests involve exposing the body to stress and measuring the response.
- Cardiac stress tests evaluate the heart during exercise.
- Allergy skin tests check the response of the skin to introduced allergens.
- Bronchial provocation testing helps with asthma diagnosis.
An overnight sleep study (polysomnography) helps diagnose sleep apnea and other sleep disorders.
Histopathology
Histopathology refers to the examination of tissue under the microscope to help diagnose and understand disease. The tissue is cut into extremely thin slices and stained with different compounds that turn different parts of the tissue different colors. A pathologist looks at the tissue under the microscope to make a diagnosis.
Cytology
After aspiration procedures, cells in the aspirated fluid are often analyzed microscopically, which is referred to as cytology.
Diagnostic Tool #6: Watchful Waiting
In watchful waiting, time and observation are used for diagnosis. The physician waits without initiating treatment to see if the disease changes its presentation. The hope is that an undiagnosable condition may become diagnosable as the disease begins producing clearer signs or symptoms.
As a familiar example, watchful waiting is the typical course of action for suspected viral upper respiratory infections (“colds”) in otherwise healthy adults. People sometimes to go urgent cares for cold symptoms, and assuming there are no red flags, the most appropriate course of action is to send the patient home to see if the infection resolves itself within 7 to 10 days. It’s not appropriate to provide antibiotics without evidence of bacterial infection, because giving antibiotics to someone with a viral infection will have no effect on their viral infection while disrupting the patient’s microbiome and contributing to antibiotic resistance.
Diagnostic Tool #7: Trial of Treatment
Sometimes, the doctor knows that a patient’s response or non-response to a particular treatment will be informative for diagnosis. A “trial of treatment” for diagnostic purposes is the administration of a treatment in a manner that will also inform diagnosis based on how the patient responds.
- If patient’s breathing gets better in response to bronchodilator treatment this suggest a diagnosis of asthma.
- If a patient’s chest pain after eating spicy food gets better with proton pump inhibitor treatment and avoiding spicy food, this suggests a diagnosis of gastroesophageal reflux.
If the diagnosis is already known by some other means—e.g., physical exam, imaging, or lab testing—then treatment is just treatment. It’s only a “trial of treatment” if the patient’s response to treatment informs the diagnostic process.
Putting it all together
A 62-year-old woman shows up at her primary care doctor’s office with a chief complaint of “feeling bad.” The doctor takes a history (tool #1), which reveals that this patient has been struggling with several months of fatigue, difficulty concentrating, low mood, weight gain, and lack of motivation. These symptoms can be seen in both hypothyroidism (low thyroid hormone) and depression.
Physical exam (tool #2) reveals thinning hair, which could be related to hypothyroidism, or merely hair loss after menopause. There are no concerning physical findings that would point to another potential cause of the patient’s fatigue and weight gain. (For example, Cushing’s syndrome can cause fatigue and weight gain, but it typically also causes other physical exam findings like central obesity with thin extremities, a rounded face, an upper back fat pad referred to as a “buffalo hump,” purple marks on the skin, thin skin, weakness of some muscles, hairiness, and/or acne. None of this is observed for the current patient.)
The doctor orders some lab tests (tool #3). A complete blood count (CBC) is normal, indicating the patient does not have anemia. A comprehensive metabolic panel (CMP) is also normal, suggesting the patient’s fatigue is not due to liver problems, kidney problems, or diabetes. Vitamin B12 and vitamin D levels are normal too. Thyroid function tests show borderline elevated TSH levels, not clearly abnormal enough for an obvious diagnosis of hypothyroidism, but not totally normal either. It is still not clear whether the patient is suffering from hypothyroidism or depression.
The doctor decides on a trial of treatment (tool #7). She prescribes levothyroxine (thyroid hormone replacement) for a couple months, and carefully monitors the patient’s energy levels, fatigue, mood, cognitive symptoms, weight changes, and repeat thyroid function tests.
Now we’ll consider two scenarios:
In one scenario, the patient feels much better taking levothyroxine. Her energy levels improve, her mental clarity returns, her mood lifts, and her TSH normalizes. This suggests she was indeed suffering from hypothyroidism, and should continue the levothyroxine.
In another scenario, the patient doesn’t feel any better on the levothyroxine. She continues having low mood, foggy thoughts, and weight gain. In this case, the patient is more likely depressed, and the doctor stops the levothyroxine and prescribes talk therapy and antidepressants.
Multiple diagnoses
Occam’s razor suggests that a single diagnosis is more likely to explain multiple symptoms than several unrelated conditions occurring simultaneously, but Hickam’s dictum says, “A patient can have as many diseases as he damn well pleases.”
The diagnostic process leading up to each diagnosis may be different.
Time to diagnosis
It may take a single clinic visit to get a diagnosis, or many years. In some cases, a diagnosis is never found. The NIH Undiagnosed Diseases Network exists specifically to conduct research on patients whose symptoms have eluded diagnosis despite extensive investigation across multiple specialties.
What’s next
A diagnosis on its own can provide clarity and peace of mind, but patients and doctors want more than that: they want the patient to get better. That’s what medical treatment is for–a topic for another day.
Diagnosis and health AI
Some health AI tools claim to “automate diagnosis” but as you can see from this post, diagnosis is complex, and there isn’t any AI system in existence today that can fully automate the whole diagnostic process for any medical specialty.
As an independent researcher (MD + AI PhD + 7 yrs prior founder/CEO experience), I build and evaluate cutting-edge healthcare AI for startups. Contact me to learn more.
Want to be the first to hear about my articles bridging healthcare, artificial intelligence, and business—and get a free list of my favorite health AI resources? Sign up here.
